By Emma Hoy
What is Pes Anserine bursitis?
Pes Anserine bursitis is an inflammation of the bursa located on the inside of the knee, just below the joint line. The Pes Anserinus is the common insertion point for three key muscles of the lower limb; Sartorius, Gracilis and Semitendinosus. This common insertion point mimics the shape of a ‘goose’s foot’, thus the translation of the name. The muscles of the Pes Anserinus primarily flex the knee but also play a stabilisation role by resisting forces applied to the outside of the knee (Lee at el., 2014).
The Pes Anserine bursa assists muscle tendon gliding by reducing friction during knee movements (Figure 1). In some circumstances, overloading one or more of the three muscles in the Pes Anserinus can result in inflammation of the bursa and a significant degree of pain. Further pain can be attributed to the separate nerve supply for each individual muscle of the Pes Anserinus (Brukner & Khan, 2012).

Figure 1. Pes Anserine muscle attachment and bursa location
Source: http://mendmyknee.com/knee-and-patella-injuries/pes-anserine-bursitis-treatments.php
Diagnosing Pes Anserine bursitis:
There are several distinct diagnostic features for Pes Anserine bursitis that your physiotherapist will confirm on examination. Key symptoms include; localised tenderness and swelling directly over the anteromedial knee, pain with resisted knee flexion and internal rotation, pain with passive hamstrings stretch and pain ascending and/or descending stairs (Rennie & Saifuddin, 2005).
Differential diagnoses of Pes Anserine bursitis
Because the Pes Anserinus is located on the medial knee, it can often be misdiagnosed due to false positive tests. Differential diagnoses include MCL sprain, medial meniscus injury, medial plica irritation and knee OA (Calmbach & Hutchens, 2003).
What causes Pes Anserine bursitis?
Pes Anserine bursitis often has a slow onset and is more commonly associated with an overuse injury, rather than the result of an acute injury. Pes Anserine bursitis occurs in response to excessive valgus strain to the medial knee structures and is thus more common in cyclists, breaststroke swimmers, runners and overweight populations (Brukner & Khan, 2012). An increase in knee valgus stress can be caused by 3 key predisposing factors;
1. Repetitive activity with poor biomechanics
Poor hip, knee or ankle stability during repetitive dynamic activities can result in an extensive amount of force going through the medial knee (Figure 2). During activities such as walking, running and jumping, poor lower limb strength and control can lead to repetitive irritation to the Pes Anserine bursa.
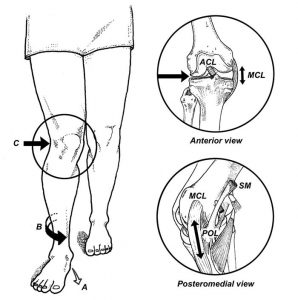
Figure 2. Strain on the medial knee with increased foot pronation and poor hip control
Source: http://blackwoodphysiosportsandspinal.com.au/hip-knee-ankle-pain/
2. Previous ligament or meniscus injury
Collateral ligament instability and medial meniscus pathologies can result in an increased demand on the Pes Anserinus to absorb excessive valgus forces placed on the knee (Figure 3).
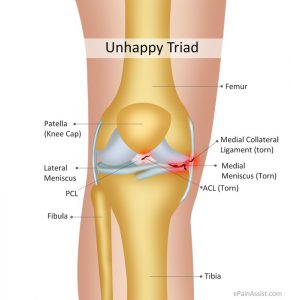
Figure 3. ACL, medial meniscus and medial collateral ligament pathology
Source: http://www.doctortierney.com/physiotherapy-blog/acl-and-the-unhappy-triad-knee-injury
3. Valgus knee deformity
Genetic variations in hip and knee alignment may predispose someone to increased risk of Pes Anserine bursitis. People with a larger Q angle (measured from the ASIS to the central patella), osteoarthritis of the medial compartment and women are more likely to have knee valgus deformity (Figure 4).
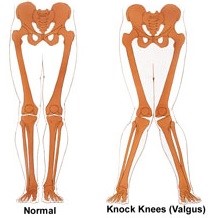
Figure 4. Knee valgus and increased stress on the medial knee.
Source: http://posturedirect.com/how-to-fix-your-knee-valgus/
How can I treat Pes Anserine bursitis?
As with all other musculoskeletal injuries, there are appropriate short-term and long-term management interventions for Pes Anserine bursitis. It is best to have your knee assessed by a physiotherapist in order to individualise a rehabilitation program.
Short-term management focuses on pain-relieving methods that include RICE (rest, ice, compression, elevation), anti-inflammatories, and electrotherapy modalities. Long-term management focuses on targeting both biomechanical and strength deficits through exercise prescription. Both stretching and strengthening exercises are beneficial for management and prevention of Pes Anserine bursitis. Below are some links to some useful exercises that can assist in early management of Pes Anserine bursitis.
Stretches:
Strengthening exercises:
1. Hamstring Isometrics
3. Split lunges (focus on knee control)
NOTE: It is advised that you consult with your local Physiohealth physiotherapist to ensure your rehabilitation is individualised to ensure optimal outcomes.
References:
Brukner, P., Khan, K., & Brukner, P. (2012). Brukner & Khan’s clinical sports medicine. Sydney: McGraw-Hill.
Calmbach, W. L., & Hutchens, M. (2003). Evaluation of patients presenting with knee pain. Part II. Am Physician, 68, 917-22.
Lee, J. H., Kim, K. J., Jeong, Y. G., Lee, N. S., Han, S. Y., Lee, C. G., … & Han, S. H. (2014). Pes anserinus and anserine bursa: anatomical study. Anatomy & cell biology, 47(2), 127-131.
Rennie, W. J., & Saifuddin, A. (2005). Pes anserine bursitis: incidence in symptomatic knees and clinical presentation. Skeletal radiology, 34(7), 395-398.