A summary and explanation of the rationale behind core stability training for acute low back pain.
Introduction Low back pain is a common disorder, with 80% percent of the population likely to experience low back pain at some stage (Walker, 2000., Ihlebaek, et al., 2006).
The causes of low back pain appear to be complex and due to many factors (Laird et al., 2012). Whilst we know there are particular structures that can contribute to pain, it is often hard to identify the primary cause, even with the use of modern day imaging (i.e MRI scanning) (Koes, et al., 2006). Despite this, there is strong research that indicate people with low back pain demonstrate changes in two major core stabilizing muscles, the Transverse Abdominus (TrA) and Lumbar Multifidus (LM) (Wong et al., 2014). Compared with individuals with no back pain, patients in pain have been shown to display diminished and delayed core muscle activity as well as reduced core muscle size. As these core muscles play such an important role in spinal control and stability, any deficits can increase the risk of low back pain (Wong, et al., 2014).
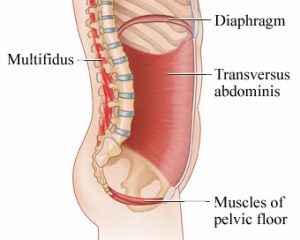
Structure & function Core stability exercise training involves the rehabilitation of the nerve and muscle systems in order to control and protect the spine and surrounding structures from injury (Hodges, 2003). The TrA muscle is a deep, corset like muscle with attachments to the lumbar spine which assist in supporting the low back (Hodges, 2003). The LM muscle is a deep muscle which lies parallel on each side of the lumbar spine which assists in control of the spinal segments whilst the body is moving (Cholewicki, 1997). Both the TrA and LM muscles are targeted by the types of exercises provided by therapists here at Physiohealth in order to create the most stable core possible.
Rationale When low back pain occurs, there are changes in the brain’s control of these core stabilizing muscles (Hodges, 2003). Once the initial muscle spasm and pain of an acute back pain episode has subsided through the use of several manual therapy techniques, a priority is to implement core stability training in order to prevent recurrence and thus promote future wellbeing. There are three distinct phases that are involved in the core strengthening programs used here at Physiohealth. The goals for each stage include:
Stage #1: Learn how to switch on your deep core muscles.
- Here the patient is provided with a simple sequence, given clear, plain instructions and uses repetition to get the hang of the contraction.
Stage #2: Challenge your deep core muscles by adding in leg and arm movements.
- The patient will here be provided with progressions in order to complicate the movement challenging the ability to maintain control of your spine and core muscles.
Stage #3: Integration into daily living and sport.
- The final stage is all about transferring your newly learnt skill into your everyday activities and sports.
Core strengthening exercises have been shown be highly effective in reducing the recurrence after an acute episode of low back pain (Ferreira et al, 2006). This is the basic rationale behind their introduction in a clinical setting at Physiohealth. The benefit of such core training programs is that under the guidance of a Physiohealth practitioner the patient can work through exercises in their own home environment after acute symptoms have been relieved. Thus working towards a happier, healthier and more active lifestyle.
Where does Pilates fit in?
Pilates training is a form of movement retraining that conditions the deep core muscles. Is it a low impact technique that focuses on controlling the core whilst performing sequenced movements of the upper and lower limbs. The complexity of the exercises is increased as you improve control and endurance. At Physiohealth we offer 30min one-on-one consultations (perfect for the beginner) and 1 hour group classes out of our Williamstown and Mount Waverly practices. Here at Physiohealth, we offer a tailored pilates program for every patient, with the overarching goal of not only returning you to your normal, pain free function, but also extending far beyond.
Further details of the specifics of the Pilates classes can be found under the services tab on the Physiohealth website. Don’t be hesitant to visit us at Physiohealth with any queries or concerns about these types of exercises or Pilates.
References: Ihlebæk C, Hansson TH, Lærum E, Brage S, Eriksen HR, Holm SH, Svendsrød R, Indahl A: Prevalence of low back pain and sickness absence: A ‘‘borderline’’ study in Norway and Sweden. Scand J Public Health 34:555-558, 2006 Walker BF: The prevalence of low back pain: A system- atic review of the literature from 1966 to 1988. J Spinal Dis- ord 13:205-217, 2000 Laird, R., Kent, P., and Keating, J., 2012. Modifying patterns of movement in people with low back pain – does it help? A systematic Review. BMC Musculoskeletal Disorders 13(169). Koes, B., Van Tulder, M., and Thomas, S., 2006. Diagnosis and treatment of low back pain. British Medical Journal, 332(7555). Wong, A., Parent, E., Funabashi, M., and Kawchuk, G., 2014. Do changes in transverse abdominus and lumbar multifidis during conservative treatment explain changes in clinical outcomes related to nonspecific back pain? A systematic review. The Journal of Pain, pp: 1-35. Hodges, P., Moseley, L., Gabrielsson, A., Gendevia, S. 2003. Experimental muscle pain changes feedforawrd postural responses of the trunk muscles. Exp Brain Res 151: 262-271. Cholewicki J, Panjabi MM, Khachatryan A. Stabilizing function of trunk flexor– extensor muscles around a neutral spine posture. Spine 1997;22:2207–12.