By Jorden Radliff
Anterior Cruciate Ligament (ACL) injuries are one of the most common knee injuries that occur in sport, especially in females with a 2-8x greater risk than males (Hilibrand et al., 2015). With such a substantial time on the sidelines these injuries can affect the athletes quality of life (QOL), sporting interaction and increase the development of post-traumatic knee osteoarthritis. There are 3 types of ACL injury mechanism, firstly contact, then indirect contact and the most common non-contact which accounts for 70% of ACL injuries (Voksanian., 2010).
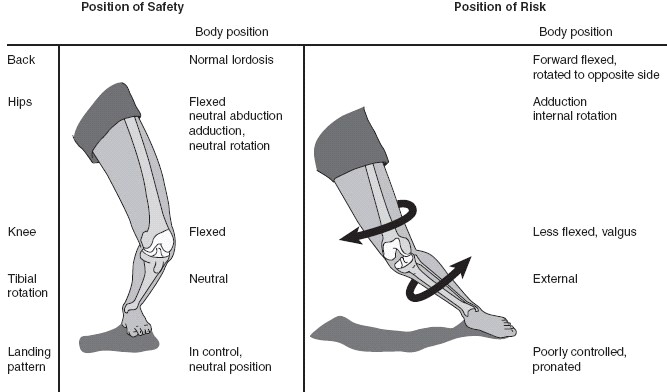
Lets briefly discuss the role of the ACL, this ligament connects the femur (upper leg) to the tibia (lower leg) and prevents the lower leg from sliding forward relative to the upper leg. Shown in the image below is the leg position that creates the greatest amount of tension on the ACL. This involves hip adducted and internally rotated, knee extended and in a valgus position and tibia internally rotated.
Currently 90% of ACL injuries are managed operatively, whilst the other 10% are managed non-operatively. Return to sport post- ACL reconstruction is said to be between 9-12 months, with a decreased risk of re-rupture every month past 9 months up to 12 months. However a larger predictor of a successful return to sport is passing all strength and control criteria measures, which can be discussed with your physiotherapist.

This is where ACL prehab plays a massive role. There is a common belief that when an athlete injuries their ACL, a physiotherapist or any health professional can’t help them until they undergo a reconstruction.THIS IS INCORRECT AND BELIEFS NEED TO CHANGE.
There is research of strong high-level evidence that pre-operative physiotherapy improves post-operative knee function and increases the chances of returning to pre-injury activity levels.
A study by Faila et al, 2016 has shown that 10 ACL prehab sessions focusing on strength and neuromuscular training resulted in improved knee function, increased quality of life and increased chances of returning to pre-injury activity levels compared to no prehab at 2 years.
Another study by Eitzen et al, 2010 stated that with a progressive 5-week exercise program prior to ACL reconstruction, significant improvements in knee function occurs, resulting in superior outcomes following ACL reconstruction.
In summary, the latest evidence has shown that both strength and neuromuscular training for a minimum of 3 weeks prior to ACL reconstruction results in superior knee function at the 12 month mark following surgery compared to ‘lets wait to see a physiotherapist after surgery’ approach. This is also true in the case of almost any impending knee surgeries. Therefore, if you have had a knee injury and suspect you may require surgery, contact your closest Physiohealth clinic to be best prepared for your recovery by undertaking a suitable pre- surgery prehab program.
Reference:
EITZEN, I., MOKSNES, H., SNYDER-MACKLER, L., & RISBERG, M. A. (2010). A Progressive 5-Week Exercise Therapy Program Leads to Significant Improvement in Knee Function Early After Anterior Cruciate Ligament Injury. The Journal of Orthopaedic and Sports Physical Therapy, 40(11), 705–721. http://doi.org/10.2519/jospt.2010.3345
Failla, M. J., Logerstedt, D. S., Grindem, H., Axe, M. J., Risberg, M. A., Engebretsen, L., … Investigation performed at the University of Delaware, Newark, Delaware, USA. (2016). Does Extended Preoperative Rehabilitation Influence Outcomes 2 Years After ACL Reconstruction?: A Comparative Effectiveness Study Between the MOON and Delaware-Oslo ACL Cohorts. The American Journal of Sports Medicine, 44(10), 2608–2614. http://doi.org/10.1177/0363546516652594
Hilibrand MJ, Hammoud S, Bishop M, Woods D, Fredick RW, Dodson CC. Common injuries and ailments of the female athlete: pathophysiology, treatment and prevention. The Physician and sportsmedicine. 2015 Nov; 43(4): 403-11. PubMed PMID: 26458108. Epub 2015/10/13. eng.
Voskanian, N. (2013). ACL Injury prevention in female athletes: review of the literature and practical considerations in implementing an ACL prevention program. Current Reviews in Musculoskeletal Medicine, 6(2), 158–163. http://doi.org/10.1007/s12178-013-9158-y