by David Cheung
Neck disorders are common (Hoy et al., 2014), painful and disabling (Haldeman et al., 2010). Out of all 291 conditions studied in the Global Burden of Disease Study (Hoy et al. 2014), neck pain ranked 4th highest in terms of disability as measured by years lived with disability. A common oversight when treating persistent neck pain is the shoulder blade (scapular). High quality literature has found specific strengthening exercises of the shoulder blade helpful in reducing neck pain (Gross et al., 2016). This article describes how it works, why it works, and gives you a step to step guide to performing “the shrug”.
The how and why
Posture and movement of the neck, shoulder and thoracic spine (mid back) are intimately related. An alteration in one region will contribute to altered movement patterns and stresses on other structures with potential to aggravate symptoms (Takasaki et al., 2009). For example, a dropped shoulder blade can cause tractional forces on muscular/joint/neural structures between the neck and shoulder (refer to figure 1). Elevation of the shoulder blade (shrug) can alleviate these stressors and potentially lead to “decompressing” the neck (Yildiz, Turgut & Duzgun, 2018). Importantly shoulder blade dysfunction is not only found in rest, but also through elevated movements i.e. swimming. I will discuss integrating swimming into the shrug later in this article.

Would this treatment suit you?
Yes, if correction of the shoulder blade provides symptom relief. This assessment can be performed by your physiotherapist (refer to figure 2).

The amount and direction of correction required depends on the position that provides you the best symptom relief. Usually[DC1] the manoeuvre involves up (shrug) and back.
Neck and thoracic gets it first
Your neck and thoracic must be assessed first by your physiotherapist prior to strengthening your shoulder blade. If indicated, your neck and/or thoracic will be treated; techniques may include massage, joint mobilization, and joint manipulation. Don’t worry, you can say no to manipulation and still get great results! Your neck may also require isolated strengthening before your shoulder blade gets it! Your physiotherapist will let you know.
Scapular exercise (the shrug)
Step 1. Setting and control
The aim of setting the shoulder blade is to be able to actively place your shoulder blade into the position proven to provide you most relief. You may need to set into down, back, up or a combination.
Which muscles am I working? Where should I feel it?
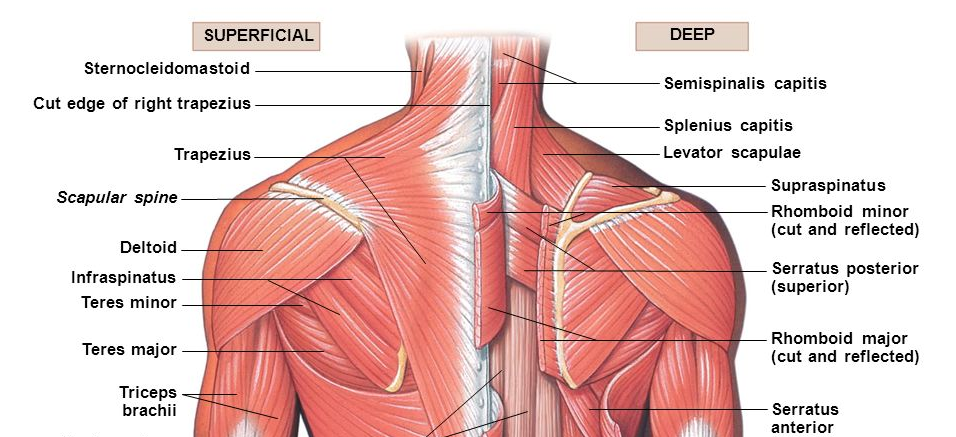
This shrug will be achieved by all the shoulder blade stabilizers, but in particular serratus anterior, upper, middle and lower trapezius (please refer to figure 3). You should aim to feel the fatigue in any of these muscles.
The aim of the shrug (refer to figure 4) is to have all the muscles activating synchronously such that a net smooth upward rotation of the shoulder blade occurs through range of motion. There is no requirement to “stop” some muscles working (such as upper traps) but rather the emphasis is on facilitating and encouraging enough firing in any muscles that may be weak, inhibited or slow to switch on in the normal movement strategies.

Perform in standing with slight abduction (30°) of the arm, in front of a mirror. Your physiotherapist will teach you the movement by applying gentle pressure to facilitate this movement. Your physiotherapist will watch for inappropriate muscle patterns.
How many do I do?
Your physiotherapist assesses how many shrugs you can achieve with good form. If repetitions of 15-20 can be achieved with fatigue and the ability to control/activate shoulder blade muscles correctly, then this is prescribed two times per day. Once for 3 sets, and another time for one set. It may be appropriate to also perform one set short of fatigue prior to sport/exercise, this is commonly known as an activation exercise.
Step 2. Progressions for strength
If control/pain/fatigue allows, you may progress by adding the resistance of rubber, commonly known as Theraband© (refer to figure 5) or by adding a weight into the hand (refer to figure 6). Resistance will facilitate greater shoulder blade activsation as well as proprioceptive feedback. Rubbers should start at yellow then red and require green if needed. Weights shoulder start at 0.5kg, progress in ½ kg increments, aiming for 3-4kgs.
0.5kg -> 1kg ->1.5kg -> 2kg ->2.5kg ->3kg ->3.5kg ->4kg.
You may progress further by combining the rubber with weights (refer to figure 7).



If you encounter increase neck pain or find the shrug too hard then they should be performed in side lying with the arm supported on a rolled-up towel (refer to figure 8).

Advanced
Progress into positions of meaninful tasks, for example, prone (on your front) for swimmers (refer to figure 9) and sitting for desk based/driving roles (refer to figure 10).


Conclusion
Neck pain may be relieved by the position and/or movement of your shoulder blade. Results show shoulder blade exercises are a safe and effective treatment in reducing neck pain. Please consult your physiotherapist before adopting the shrug.
References
Gross, A. R., Paquin, J. P., Dupont, G., Blanchette, S., Lalonde, P., Cristie, T., . . . Bronfort, G. (2016). Exercises for mechanical neck disorders: A Cochrane review update. Man Ther, 24, 25-45. doi:10.1016/j.math.2016.04.005
Haldeman, S., Carroll, L., & Cassidy, J. D. (2010). Findings from the bone and joint decade 2000 to 2010 task force on neck pain and its associated disorders. J Occup Environ Med, 52(4), 424-427. doi:10.1097/JOM.0b013e3181d44f3b
Hoy, D., March, L., Woolf, A., Blyth, F., Brooks, P., Smith, E., . . . Buchbinder, R. (2014). The global burden of neck pain: estimates from the Global Burden of Disease 2010 study. Annals of the Rheumatic Diseases, 73(7), 1309. Retrieved from http://ard.bmj.com/content/73/7/1309.abstract. doi:10.1136/annrheumdis-2013-204431
Takasaki, H., Hall, T., Jull, G., Kaneko, S., Iizawa, T., & Ikemoto, Y. (2009). The influence of cervical traction, compression, and spurling test on cervical intervertebral foramen size. Spine (Phila Pa 1976), 34(16), 1658-1662. doi:10.1097/BRS.0b013e3181a9c304
Yildiz, T. I., Turgut, E., & Duzgun, I. (2018). Neck and Shoulder blade-Focused Exercise Training on Patients With Nonspecific Neck Pain: A Randomized Controlled Trial. J Sport Rehabil, 27(5), 403-412. doi:10.1123/jsr.2017-0024