By Ksaniel Hasanki
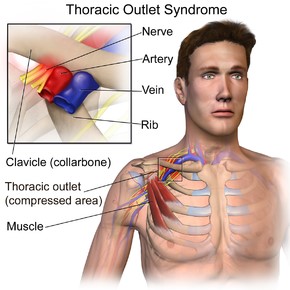
The term thoracic outlet syndrome (TOS) refers to a group of conditions that result from compression of neurovascular structures (nerves and blood vessels) that course from the neck to the axilla (armpit) through the thoracic outlet. The nerves in the brachial plexus and sub-clavian artery and vein are especially susceptible to compression because of their proximity to one another in the thoracic outlet. There are three types of TOS which represent the site and structures being compressed.
Sub-Categories:
1) Costoclavicular Syndrome
A compression of structures at the space between the clavicle/collar bone and the first rib and is the most common site of compression.
2) Anterior Scalene Syndrome
Compression of the triangular space between the anterior and middle portion of the scalene muscles at the front of the neck, and the upper portion of the first rib.
3) Pectoralis Minor or Hyper-abduction Syndrome
Pectoralis minor syndrome is considered if there is also a compression between the coracoid process and the pectoralis minor muscles attachment to the ribs
Symptoms:
• Pain in the neck or shoulder
• Numbness in the upper limb, forearm or hand
• Tingling in the upper limb, forearm or hand
• Feeling of weakness in the arm
• Easily fatigued arm
• Decreased pulse rate in wrist compared to neck
Not all the above symptoms need to be present to have TOS. Patients may present with varying combinations of symptoms which will indicate the type of TOS they have. Most commonly symptoms are mixed and not purely arterial, venous or neurogenic in nature.
This condition most commonly occurs in overhead athletes and people with poor posture and drooping shoulders. Individuals with shoulder blade protraction can experience TOS symptoms by compressing the canal through which the neurovascular structures pass through. Anatomical abnormalities including extra bones or tissue such as a complete cervical rib, incomplete cervical rib with fibrous bands, fibrous bands from the transverse process of the C7 vertebra, and collar bone abnormalities, can also compress the neurovascular structures. Complete cervical ribs are rare but, if present are often bilateral and only affect about 10% of patients.
Traumatic structural changes that can cause TOS include fractures of the collar bone and/or first rib, malunion of clavicle fractures, callus formation or a crush injury of the upper thorax. TOS symptoms are common in patients with chronic scapular dysfunction. A typical patient will have tight pectoralis minor, scalene and upper trapezius muscles, with weak serratus anterior and lower trapezius muscles; causing excessive anterior tilt and protraction of the scapulae.
Treatment:
Treatment for any subset of TOS focuses on the specific area compromised. However, certain treatments apply to all forms of TOS. Correction of drooping shoulders, poor posture and poor body mechanics is vital. The patient should be taught proper positioning while sitting, standing and lying down. Physiotherapy will include pectoral and scalene stretching and trigger point treatment, along with soft tissue mobilisation of restricted tissues as well as scapular and scapulothoracic mobilisation. Joint mobilisation of the first rib can restore accessory motion of the sternoclavicular and acromioclavicular joints. Therapeutic exercise, education and manual therapy can correct forward head posture.
Surgical consultation and treatment is warranted for patients who have neurogenic TOS that does not respond to aggressive conservative management and for patients who have vascular compromise or thrombus/clot formation however your physiotherapist will be able to further advise on this.
If you have any of the symptoms listed above please be sure to contact your nearest Physiohealth clinic to receive an expert assessment for an accurate diagnosis and appropriate treatment strategy for your condition.